Quick Answer
- Driver A: AHI dropped from 108.1 to 13.5 (about 87%) on a custom oral appliance alone. Time below 85% oxygen fell from 43.5 minutes a night to zero. No CPAP machine involved.
- Driver B: AHI dropped from 60.5 to 4.7 (about 92%), landing in the normal range. REM sleep climbed from 2.3% to 29.8%.
- What it means: Neither needed a federal AHI "pass" number, because there isn't one. The goal was breathing controlled enough to satisfy a DOT examiner without a mask, and both got there.
Informational only, not medical or legal advice. These are real, de-identified results from two patients. Your apnea, your anatomy, and your DOT status are individual. Decide with a sleep physician and your FMCSA-certified medical examiner.
Table of Contents
- Quick Answer
- Why I'm Sharing These Two Cases
- How to Read These Charts
- Driver A: From 108.1 to 13.5 Without a Mask
- Driver B: From 60.5 to 4.7, Into the Normal Range
- What These Numbers Mean for a DOT Exam
- Why This Worked Without CPAP
- The Honest Limits: Who This Is Not For
- What the FMCSA Actually Requires
- Your Next Step
- Frequently Asked Questions
- Sources & Further Reading
Why I'm Sharing These Two Cases
I treat my own sleep apnea with an oral appliance, so I don't talk about this work from a distance. But I also know that promises are cheap. Every clinic on the internet says it gets great results. So instead of telling you what an oral appliance can do, I want to show you, with two real sleep studies from drivers I treated.
To protect their privacy, I've stripped every identifier. No names, no dates, no birthdays, nothing that could point back to a person. I'll call them Driver A and Driver B. What you're seeing below are the actual before-and-after charts from their sleep tests, the same numbers their doctors and DOT examiners saw. These results are already published on our CPAP alternative results page; this article walks through what they mean for someone trying to keep a CDL.
Both men came to me in the same spot: a serious diagnosis, a CPAP they couldn't keep on their face in a sleeper cab, and a real fear about their medical card. Here's what happened.
How to Read These Charts
If sleep-study numbers are new to you, here are the only two you really need:
- AHI (apnea-hypopnea index): the average number of times an hour your breathing stops or goes shallow. Under 5 is normal. 5 to 15 is mild. 15 to 30 is moderate. Over 30 is severe.
- Oxygen saturation (O2): how low your blood oxygen drops while you sleep. Long stretches below 88 to 90% are the dangerous part, that's your heart and brain getting starved of oxygen, over and over, all night.
A "before and after" sleep study simply measures these on your worst night versus a night on treatment. Lower AHI and steadier oxygen mean the airway is staying open. Watch what happens to both.
Driver A: From 108.1 to 13.5 Without a Mask
Driver A had what we call very severe obstructive sleep apnea. His AHI was 108.1. Read that again: his breathing was collapsing roughly 108 times an hour, nearly twice a minute, every minute, all night long. He was waking up exhausted no matter how long he stayed in the bunk, because his body never got to do the deep work of sleep. His REM sleep, the restorative stage, was a starved 6.4% of the night.
He'd been handed a CPAP and, like a lot of drivers, couldn't live with it on the road. By the time he reached me he was scared he was going to lose his card, or worse, fall asleep at the wheel.
Here is his AHI, before and after a custom oral appliance:
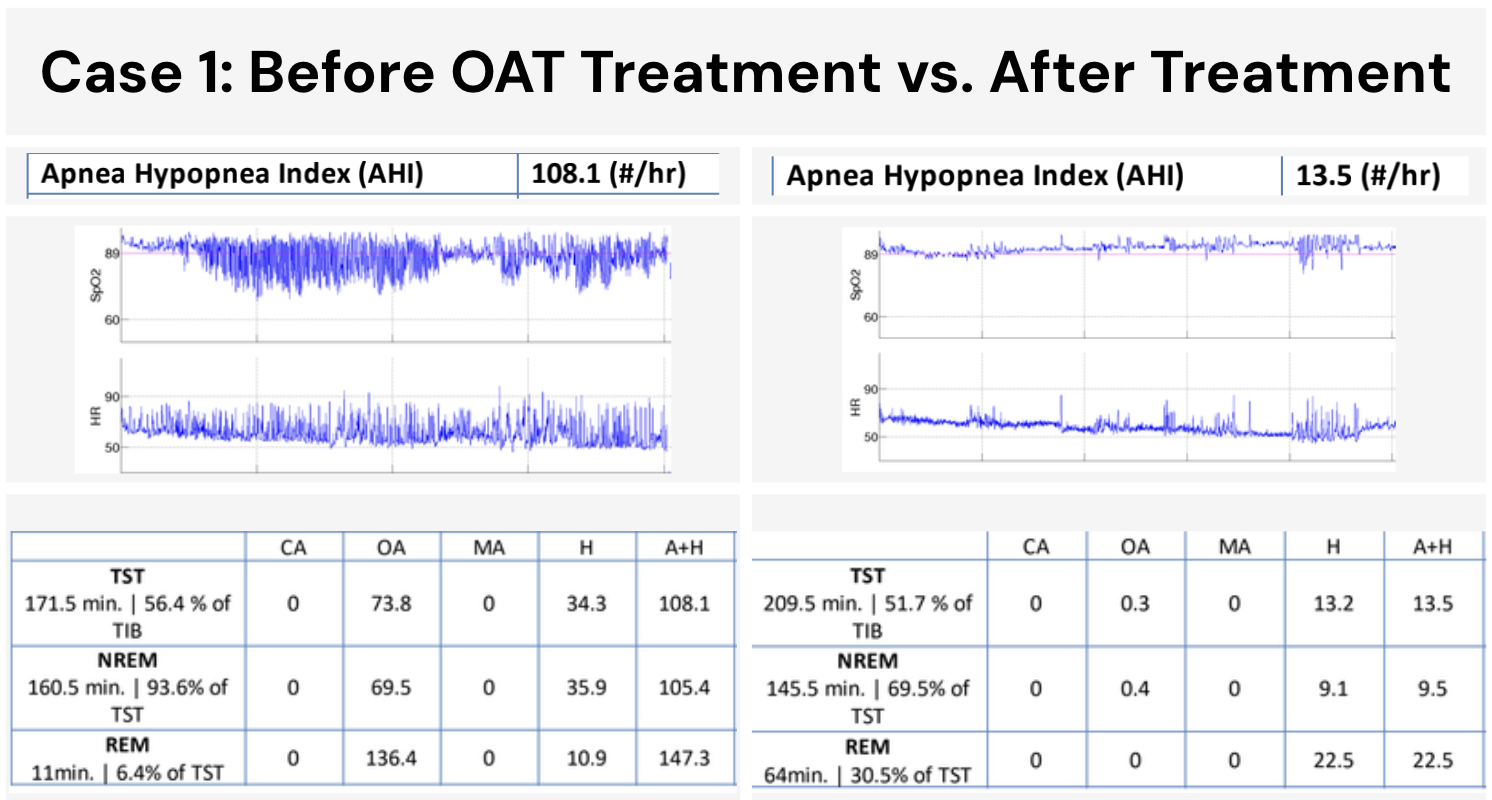
His AHI fell from 108.1 to 13.5. That's about an 87% reduction, taking him from the most severe category all the way down into the mild range, on an appliance alone, with no machine, no mask, no hose.
But the AHI isn't even the part that moves me most. Look at his oxygen:
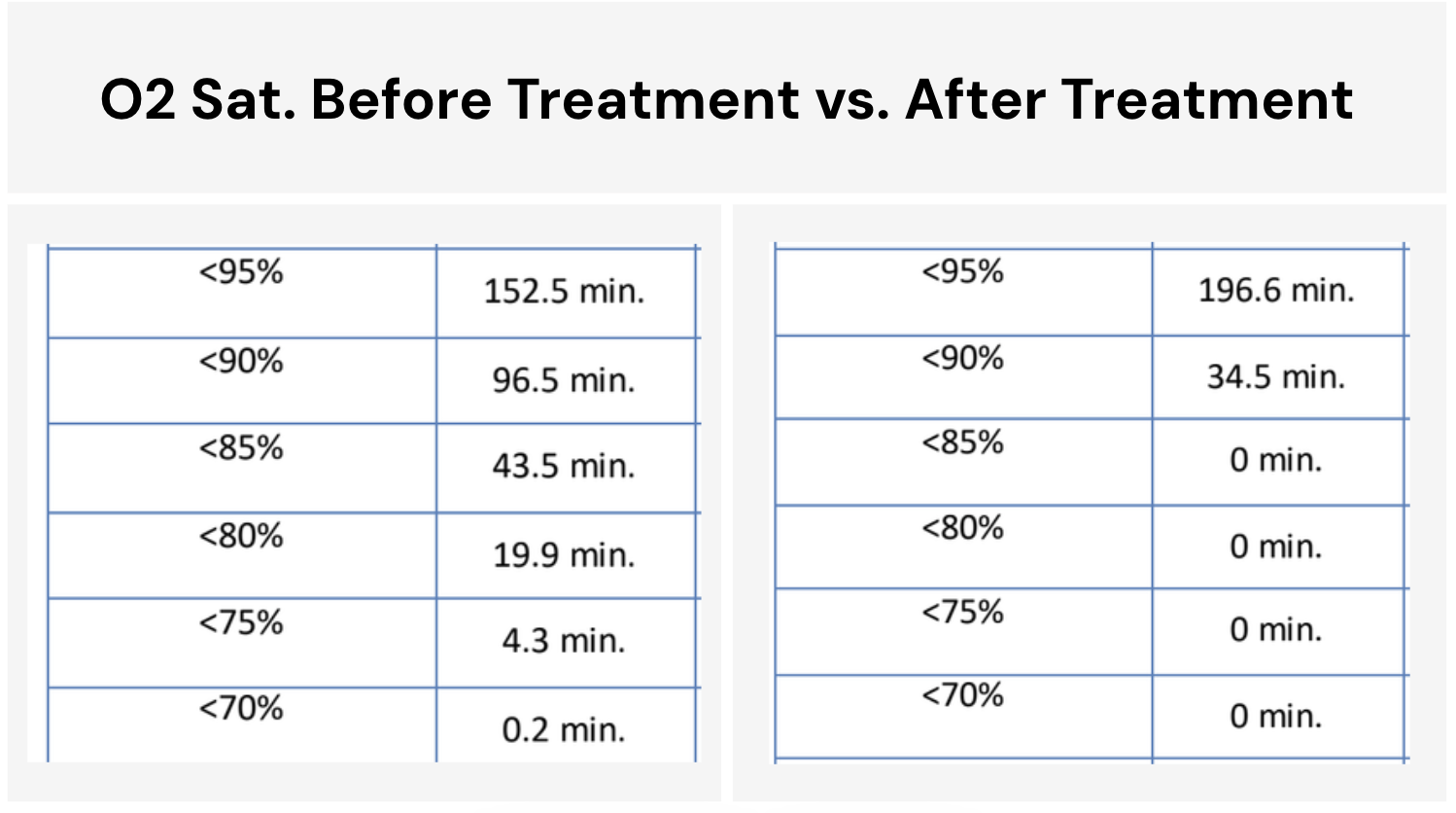
Before treatment, he spent 43.5 minutes of the night with his blood oxygen below 85%. Forty-three minutes of his body suffocating in slow motion, night after night. After the appliance: zero minutes below 85%. And his REM sleep climbed from 6.4% to 30.5%, almost five times more restorative sleep.
This is one man's result, and an unusually strong one for apnea this severe. I'm not promising you'll match it. But I'm showing it to you because a lot of drivers are told that severe apnea means "CPAP or nothing," and that simply isn't always true.
Driver B: From 60.5 to 4.7, Into the Normal Range
Driver B's apnea was severe too, an AHI of 60.5, about 60 breathing events an hour. His REM sleep was almost nonexistent at 2.3%. He described the exact thing I hear constantly: years of dragging through the day, blaming "the life," not realizing a treatable condition was stealing his sleep.
Here's his before-and-after AHI:
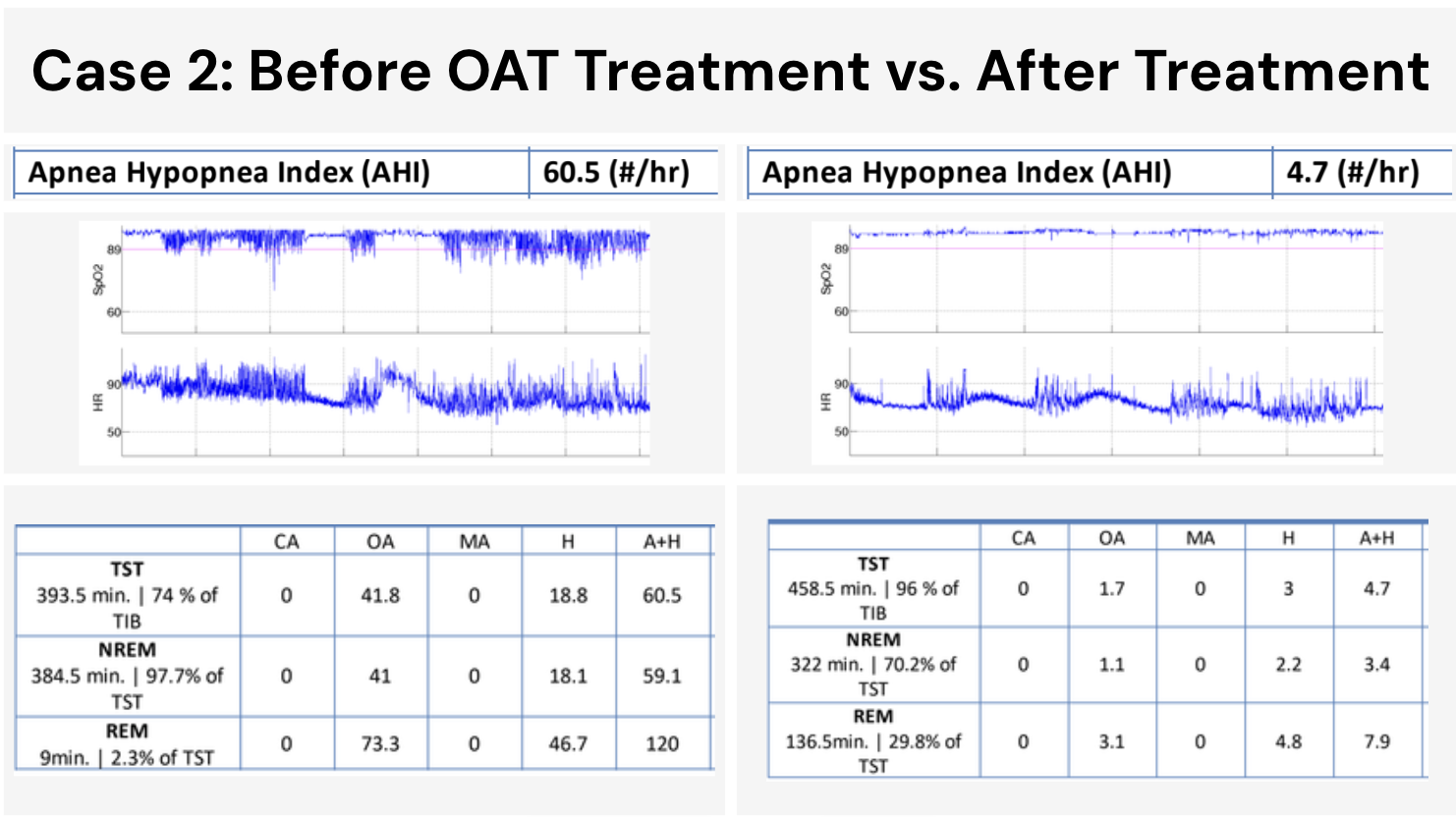
His AHI dropped from 60.5 to 4.7, about a 92% reduction. That 4.7 is the number that matters: it's below 5, which is the normal, non-apneic range. On a custom oral appliance, this driver went from severe sleep apnea to a normal sleep study.
And his oxygen tells the same story of an airway that finally stayed open through the night:
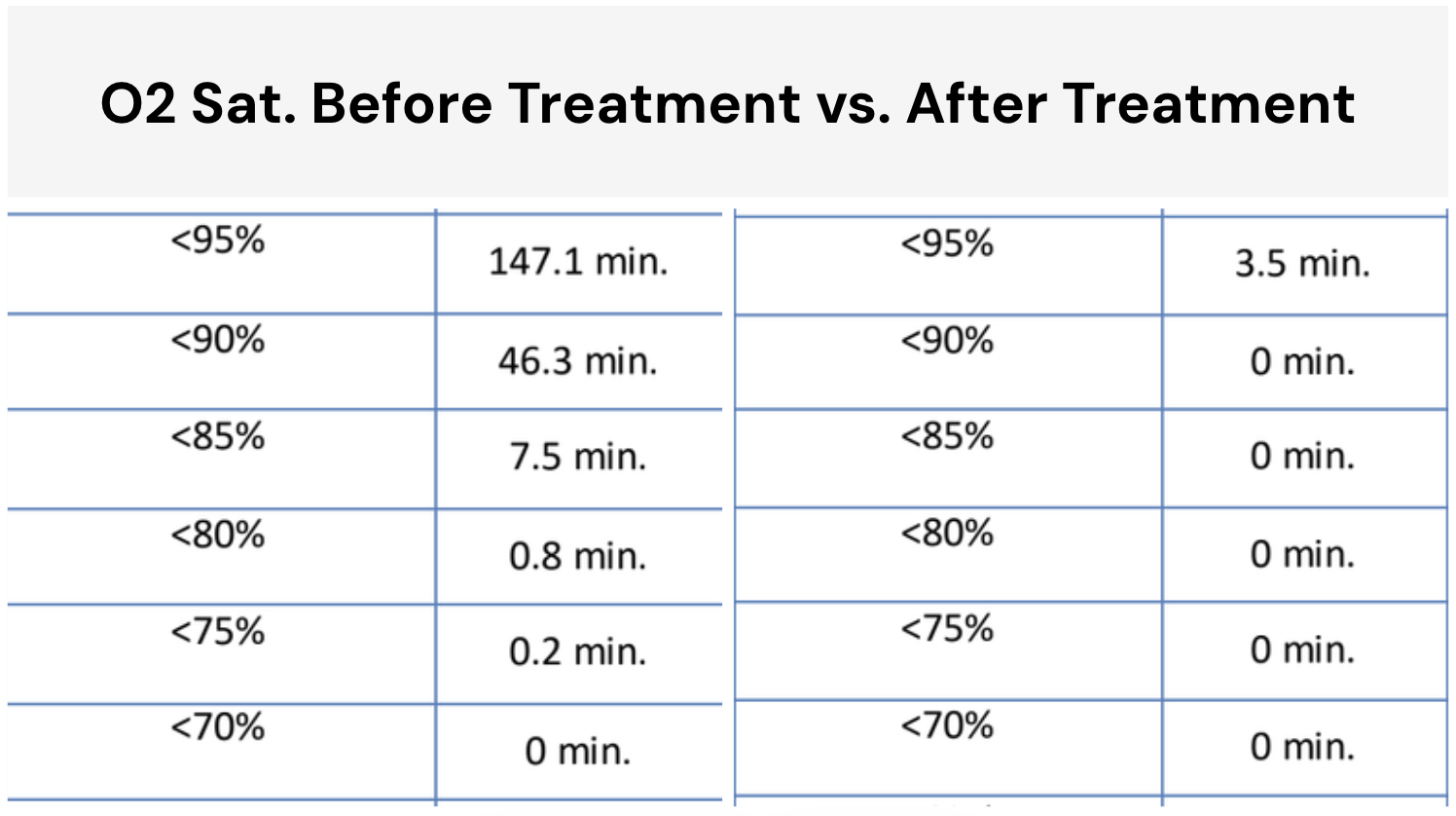
His REM sleep recovered from 2.3% to 29.8%, a normal, healthy amount. For the first time in years, his body was getting the sleep it had been starving for.
What These Numbers Mean for a DOT Exam
Here's where drivers get tripped up, so let me be precise. There is no federal AHI number you must hit to keep your CDL. People repeat "you need to be under 20" or "under 15" as if it's law. It isn't. The FMCSA Medical Examiner's Handbook does not set a national apnea cutoff, and it does not require any specific device.
What it does is leave the decision to your certified medical examiner's clinical judgment. The examiner wants to see two things: that you're diagnosed, and that you're being treated effectively, with documentation to prove it.
So why do these before-and-after numbers matter so much? Because they are the documentation. When Driver B walks into his physical with a follow-up sleep study showing an AHI of 4.7 on his appliance, his examiner isn't guessing. The proof is right there: controlled breathing, restored oxygen, real treatment. That's what supports certification.
For an oral appliance specifically, the proof your examiner wants is a follow-up sleep test taken with the device in your mouth, showing your breathing events are controlled. That's exactly what the charts above are. (For the full certification playbook, see DOT sleep apnea requirements and how to keep your CDL with sleep apnea.)
Why This Worked Without CPAP
A custom oral appliance is a precision dental device, worn only during sleep, that holds your lower jaw slightly forward. That small shift pulls the base of your tongue away from the back of your throat and keeps the airway from collapsing. No air pressure, no mask, no machine.
For these two drivers, three things made the difference:
- It was custom and titrated, not a drugstore guard. I took digital impressions, fit a medical-grade device, and then advanced it gradually over several weeks to find the exact position that controlled their breathing. A boil-and-bite sport guard can't do that and shouldn't be used to treat apnea.
- They actually wore it. This is the quiet secret of the whole field. The best treatment is the one you use every night. A 2013 randomized trial found CPAP and oral appliances produced similar real-world health outcomes, because people wear the appliance more consistently (Phillips et al., 2013). A device in your mouth beats a machine in a bag.
- We retested to prove it. We didn't assume it worked. We measured. That follow-up study is both the medical confirmation and the DOT documentation, in one.
The Honest Limits: Who This Is Not For
I'd be doing you a disservice if I only showed you the wins. So here's the straight talk.
Driver A's result, severe apnea controlled by an appliance alone, is real but not typical. Oral appliances are most predictable for mild-to-moderate apnea. The more severe the disease, the harder it is for an appliance to fully control it, and the more likely you'll need CPAP or a combination approach.
An oral appliance is probably not your answer if:
- You have central or complex sleep apnea. An appliance opens a blocked airway. It can't fix apnea that comes from the brain's breathing signals. That's CPAP or specialized therapy.
- Your apnea is very severe and you tolerate CPAP well. If the mask works for you, it's the most-studied, first-line treatment for severe disease. Don't fix what isn't broken.
- You don't have enough natural teeth or implants to anchor the device securely. Full dentures on both arches usually rule it out.
The point of these two cases isn't "appliances beat CPAP." It's that for the right driver, an appliance you'll actually wear can get your numbers, and your DOT documentation, exactly where they need to be. The honest move is matching the device to your apnea, your anatomy, and your route, with a sleep physician, not picking a side from a blog.
What the FMCSA Actually Requires
Let me clear up the rules one more time, because bad internet advice scares good drivers out of getting help.
There is no federal AHI threshold. The FMCSA Medical Examiner's Handbook (2024 edition) sets no national apnea number that disqualifies you. Certification is at your examiner's discretion.
The 2016 rule is dead. FMCSA and the Federal Railroad Administration floated a sleep-apnea rule in 2016 and withdrew it in August 2017. There is no special federal apnea regulation hanging over drivers today.
Examiners certify treated drivers. Diagnosed and following effective treatment, with proof, is what keeps your card. Hiding the problem until a fatigue event is what loses it.
Your Next Step
If you've been white-knuckling your alertness on long hauls, or you tried CPAP and quietly gave up, the two drivers above were once exactly where you are. A serious diagnosis. A mask they couldn't keep on. A real fear about the card that feeds their family.
They didn't have to choose between sleeping safely and keeping their livelihood. The right treatment protected both. My own family knows what untreated apnea behind a wheel can cost, so this isn't a slogan to me.
The only way to know your number is to measure it. A home sleep test can tell you where you stand, and a follow-up test can prove your treatment works to the examiner who holds your card.
Get a DOT sleep test and let's find out what your before-and-after could look like.
With respect for the miles you carry,
Dr. Henry Qiu Wakewell Sleep Wellness
P.S. If a previous CPAP "failure" is haunting you, set it down. Most drivers who couldn't tolerate CPAP do well with a custom oral appliance. The road has a treatment that fits it, and we can find yours.
Dr. Henry Qiu is a UCLA-trained dental sleep medicine specialist focused on custom oral appliance therapy and whole-airway care. He manages his own sleep apnea with an oral appliance and helps commercial drivers stay rested, certified, and safe behind the wheel. The case results shown here are real and de-identified; individual results vary.
Sources & Further Reading
Phillips CL, et al. (2013), American Journal of Respiratory and Critical Care Medicine: Randomized controlled trial finding CPAP and oral appliance therapy produced similar real-world health outcomes despite CPAP's greater efficacy. Read the study
Ramar K, et al. (2015), Journal of Clinical Sleep Medicine (AASM/AADSM joint clinical practice guideline): Recommends oral appliance therapy for adults with OSA who are intolerant of CPAP or prefer alternate therapy. Read the guideline
Weaver TE & Grunstein RR (2008), Proceedings of the American Thoracic Society: Review documenting that roughly half of CPAP users do not maintain adequate adherence. Read the review
FMCSA Medical Examiner's Handbook, 2024 Edition: Confirms OSA certification is at examiner discretion with no mandatory federal AHI threshold or required device. Read the handbook
FMCSA & FRA (2017), Federal Register: Official withdrawal of the 2016 obstructive sleep apnea advance notice of proposed rulemaking. Read the notice